Syndemics consider where two or more conditions cluster together, how these conditions interact, and what drives these conditions to cluster and interact in the first place. Many people frame syndemics by considering disease concentrations and disease interactions. In this way, understanding where and how co-occurring diseases emerge requires that we take stock of what drives them. For example, this might be due to environmental changes or escalating wealth inequality in rich and poor countries alike. It could also involve corporations that flood markets with cheap, easy to access oily, sugary, and salty foods that impede healthier options from the menu, therefore fueling an illusion of choice. Notably, history, society, culture, ecology, economy, and politics play important roles not only in driving what diseases are diagnosed in the clinic but also how people experience them. We have explored these questions across various contexts and found that syndemics differ in meaningful ways in Kenya, South Africa, Ethiopia, India, and the United States, despite the clustering of similar medical conditions.
We have spent years investigating what it means to live with multiple morbidities in Soweto, South Africa—a township of more than one million people in Johannesburg. Most of our research was conducted in IsiZulu, a common language spoken in Soweto, as well as English. Building on multiple research projects with patients diagnosed with chronic conditions like type 2 diabetes, hypertension, HIV, cancer, cardiovascular disease, chronic pain, anxiety, and depression, we designed a survey that encompassed many of the ways in which people experienced and coped with stress in their lives. We found that this scale was effective at showing who might express more distress than others. This ethnographically grounded scale is what we used to study “stress” in our analysis of syndemics. However, we spent hours learning from our participants about how they defined good health and a good life on their own terms, too.
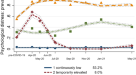
In our recent Nature Human Behavior paper, we showed how impactful social stress was on quality of life among people living with multiple chronic medical conditions. People we interviewed at length talked more about the social and structural challenges that hindered them from taking care of their illnesses, as opposed to the illnesses themselves. We used a sophisticated multiple step and multi-method approach to define the terms in which people experienced and responded to stress as well as how those stresses affected chronic illness. Our quantitative analyses with a population-based sample of nearly one thousand people demonstrated that social stressors can undermine one’s quality of life more than living with multiple chronic conditions. We found that people who experienced less social stress were more likely to report higher quality of life regardless of the number of chronic conditions they reported to have or were diagnosed with. In this way, we showed how the social dimensions of the syndemic were more influential on one’s health than medical ones.
For example, we interviewed 30 people from our large sample about what it means to live a good life in Soweto, or being well (inhlalakahle in IsiZulu). We described how Thulasizwe lives a flourishing life despite having been diagnosed with type 2 diabetes, hypertension, and epilepsy. He faced multiple struggles and in his darkest times was comforted by loved ones. However, he describes how he overcame these diagnoses and early years of chronic illness by sharing his gifts with others and a staunch determination and perseverance to be and do well. In this way, he describes how the concept of ubuntu—defined as I am a person because of other people—is crucial to him living a good life. A related term in IsiZulu is umuntu owaphumelela (meaning, someone who has flourished). In contrast, another participant, Naledi, described how the most distressing experience in her life was not a medical condition but rather shunning by elders. In this way, the social aspects of life were central to living a good and healthy one.
We also found God, spirituality, and the church were essential in how people adjusted and coped with both medical and social challenges. This is not surprising given the common practice of evangelical Christianity in Soweto. For example, people who engaged in religious practices such as worshipping together, reading the holy texts, praying, personal faith, and spirituality demonstrated better coping strategies amidst everyday social, moral, and medical challenges than those who were not daily practitioners. In addition, an intimate relationship with God was said to be more important in people’s lives when compared to relying on overcrowded and under-resourced hospitals and clinics in Soweto, where many people felt unheard, ignored, silenced, or misunderstood. Other social networks such as family, friends and neighbors were described as crucial in people’s self-management of multiple cascading health conditions. People who experienced less stigma and mistreatment from family, caregivers or neighbors, also struggled more.
Disentangling causality of what caused people to become sick and populations to disproportionately suffer from multiple morbidities remains opaque in part because the cause is a confluence of history, politics, society, and policy. Recognizing how crucial social relations are to how people live well with illness, however, is clear. Our research underscores the importance of not only patient-centered care but also of un-centering the hospital as the primary point of care-giving and considering how healthy lives can be promoted by investing in religious contexts, families, and places where people seek, receive, and foster good physical and mental health.
Authors listed alphabetically
Edna N. Bosire, PhD, is a medical anthropologist and post-doctoral fellow at the Center for Innovation in Global Health, Georgetown University and Kamuzu University of Health Sciences, Mahatma Gandhi in Blantyre, Malawi. Dr. Bosire is honorary faculty at South African Medical Research Council (SAMRC)/Wits Developmental Pathways for Health Research Unit in the Faculty of Health Science in Johannesburg, South Africa.
Lindile Cele, MSc, is a research associate at South African Medical Research Council (SAMRC)/Wits Developmental Pathways for Health Research Unit in the Faculty of Health Science at the University of the Witwatersrand in Johannesburg, South Africa.
Emily Mendenhall, PhD, MPH, is a medical anthropologist and professor at Georgetown University’s Walsh School of Foreign Service. She serves as honorary faculty at South African Medical Research Council (SAMRC)/Wits Developmental Pathways for Health Research Unit in the Faculty of Health Science at the University of the Witwatersrand in Johannesburg, South Africa. Her newest book is Unmasked: COVID, Community, and the Case of Okoboji.



Please sign in or register for FREE
If you are a registered user on Research Communities by Springer Nature, please sign in